Malaria, dengue, chikungunya, schistosomiasis, and other vector-borne diseases account for more than 17% of the global infectious disease burden, killing over 700,000 people each year.1
In the case of Chikungunya, it is a mosquito-borne viral disease caused by RNA virus. The virus was first discovered in Tanzania in 1952 and has caused occasional outbreaks since then in Africa and Asia.2 The reason is its habitat. The prevalence of Chikungunya is highest in the warm tropical and subtropical areas, which are the natural habitats of mosquitos. In the absence of the required sanitation and other preventive measures, it disproportionately affects the poorest populations.1
It may claim lives and cause chronic suffering, life-long morbidity, and even disability.1 Moreover, a large proportion of the infected patients suffer from post-infection sequelae of chikungunya. Infected newborns and elderly people with comorbidity are at high risk of developing the associated complications.3
In the following blog, we shall discuss the post-epidemic sequelae of Chikungunya, a vector- borne disease.
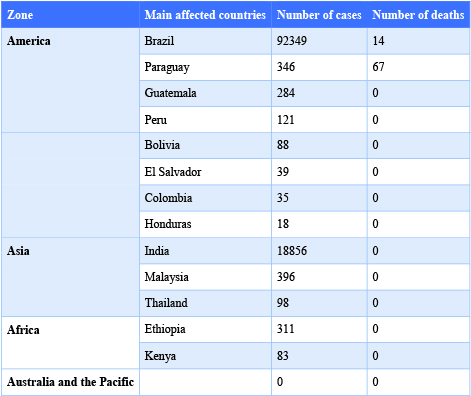
Source: European Centre for Disease Prevention and Control.
The incubation period of the disease can range from 2–12 days after being bitten by an infected mosquito. The most common symptoms and the associated complications are shown in the box below.2
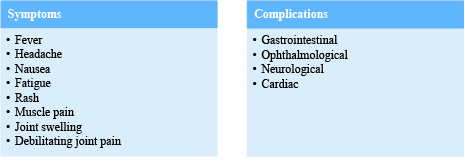
Complications can occur in occasional cases, especially in the elderly with other co-morbid conditions. However, most patients recover completely and get life-long immunity to the virus.
But in some cases, debilitating joint pain may last for a few days, weeks, months, or even years and progress to arthritis.2
The first case of a post-chikungunya rheumatic disorder was reported in South Africa after an outbreak in the 1970s.5 Let us look at a few case studies to better understand these complications.
A case study from Thailand reported that a Thai woman in her mid-forties returned to the Fever Clinic at Bangkok Hospital for Tropical Diseases almost a year after being cured of Chikungunya. The patient had a fever, chills, arthralgia, and unilateral swelling and stiffness in her left hand. There was swelling, erythema, and tenderness to palpation of the flexor surfaces of her fingers in the affected hand.
The swelling extended from the proximal interphalangeal joints to the metacarpophalangeal joints. It produced stiffness in her fingers, limiting their range of motion. Hence, the execution of her day-to-day activities was adversely affected. However, the patient had no underlying past medical history of diabetes, hypertension, chronic lung disease, chronic kidney disease, ischemic heart disease, or any known musculoskeletal disorder and was not consuming any medications or supplements.5
In contrast, in another observational and longitudinal study conducted at the rheumatology department in Neiva, Huila. In this study, data was collected from 410 patients infected with the CHIKV virus. The average age of study subjects was 57.3±11.7 years. Data was retrospectively analyzed using a simple linear regression analysis using SPSS (Statistical Package for Social Sciences) to identify the risk factors for the development of pCHIKV RA (post chikungunya rheumatic arthritis). The findings are summarized in Figures 1 and 2 below.6
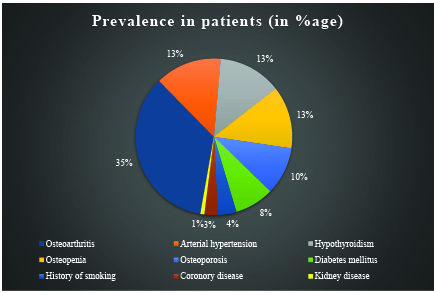
Thus, it can be inferred from the chart above that post-chikungunya arthritis is more prevalent in people with pre-existing diseases like osteoarthritis, osteoporosis, osteopenia, rheumatoid arthritis, and a family history of rheumatic disease.
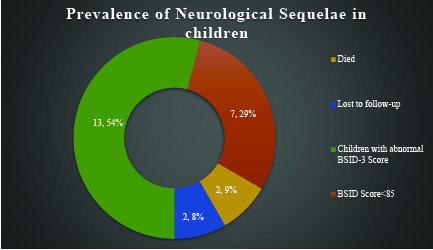
Yet another case study was conducted to examine the neurologic sequelae of severe chikungunya infection in the first 6 months of life of infants. The findings are shown in the pie chart below.
The mean BSID-III cognitive score for children was 84.71 (N = 17; SD 7.4), indicating mild cognitive impairment. But none of the study subjects had a cognitive composite score of less than 70, showing that the cognitive ability of children was not moderately or severely impaired.7
From the above case studies, it can be inferred that both arthritis and neurological complications are associated with chikungunya. While the cause of neurological complications is not yet understood completely, post-CHIKV inflammatory arthritis is characterized by the expression of pro-inflammatory cytokines and chemokines similar to those found in rheumatoid arthritis. Yet the patients were seronegative for rheumatism. Moreover, age-related interferon dysfunction may have a role in the peripheral articular joints that are most commonly engaged in CHIKV infection. Furthermore, the existence of co-morbid diseases may have a key role in the development of post-CHIKV inflammatory arthritis.5
pCHIKV-RMSD can be diagnosed with serological tests, such as enzyme-linked immunosorbent assays (ELISA) and reverse transcriptase–polymerase chain reaction (RT–PCR). These tests detect the presence of viruses, viral nucleic acid, or IgM and IgG anti-chikungunya antibodies in the serum samples.2 Clinical manifestations supported by positive test findings help in establishing a diagnosis of pCHIKV-RMSD.
However, no specific antiviral drug treatment is available for chikungunya. The clinical management of cases is limited to relieving the symptoms, including joint pain, using antipyretics, optimal analgesics, anti-inflammatory drugs, and physiotherapy.13 Drinking plenty of water and taking adequate rest can also help such patients.2 Yet several vaccines are in different phases of clinical testing for evaluation of their safety and efficacy. Some of them include:
The above discussion reveals that significant progress has been made in understanding the pathogenesis of post-CHIKV inflammatory arthritis. However, more study is needed to understand the etiology of this disease’s neurological complications and to develop effective preventive and therapeutic measures to treat this disease. Furthermore, proper sanitation and vector control measures can assist in the prevention of future outbreaks of chikungunya.
Reviewer: Priyanka
Copyright © 2025 All Rights Reserved