Over the last two decades, coronaviruses such as Severe acute respiratory syndrome coronavirus (SARS-CoV), Middle East Respiratory Syndrome Coronavirus (MERS-CoV), and SARS-CoV2 have wreaked havoc on our planet, posing global health threats and leaving death, misery, and suffering in their wake. The situation has been worsened by the tremendous economic impact worldwide.1 It has led to inflation and supply chain disruptions.2 Moreover, the circulation of misinformation has caused massive panic in the masses. But are all coronaviruses really as infectious and as deadly as they are rumored to be? Let’s discuss the MERS-CoV virus in detail.
Several MERS-CoV outbreaks have been documented in Asia since its discovery in the Kingdom of Saudi Arabia (KSA) in 2012. In 2014, 255 laboratory-confirmed cases (including 40 healthcare personnel) and 93 deaths were recorded in an outbreak in Jeddah.3 In fact, 939 cases of MERS-CoV were reported in KSA from 2012–2015.4 In 2015, the largest MERS outbreak outside of the Middle East was reported in the Republic of Korea, with 186 laboratory-confirmed cases and 38 deaths.5
This blog outlines the predominant characteristics of MERS concerning demographics, transmission, clinical manifestations, risk factors, and laboratory and radiology findings.
MERS-CoV usually infects the lower respiratory tract. It has a broad clinical spectrum, resembling many other bacterial and viral lung infections. The infection is mostly transmitted through contact with infected dromedary camels. However, infrequent human-to-human transmission can also occur.1 Particularly in healthcare facilities where infection control protocols are rarely followed while the patient is receiving care.6
Even though MERS-CoV is significantly less contagious than SARS-CoV and SARS-CoV2, its Case Fatality Rate (CFR) (nearly 40%) in symptomatic patients is significantly higher when compared to SARS-CoV-2 (10.87%). Moreover, there are no approved preventive and therapeutic measures available to combat this disease. Hence, the World Health Organization (WHO) included it in its annual R&D blueprint list of prioritized pathogens for accelerated
research and development in diagnostics, vaccines, and therapeutics in 2015.7 Besides, MERS is suspected to have the potential to cause an epidemic worldwide.
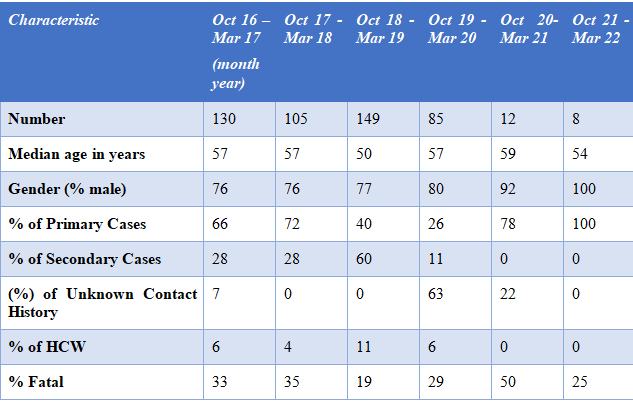
By the end of March 2022, a total of 2589 laboratory-confirmed cases of MERS, including 893 associated deaths, had been recorded globally. Of these, 2184 MERS cases, including 813 related deaths, were reported from Saudi Arabia. In addition, the disease has spread throughout the world, with cases being reported in 27 other countries, including the United Kingdom and the United States of America. However, all reported cases either lived in or traveled to the Arabian Peninsula before falling ill. A few of them had close contact with the infected travelers.
But why should we consider this data? The epidemiological data helps scientists to understand the transmission process and, thereby, detect the occurrence of outbreaks promptly, allowing them to be better prepared to handle epidemics. The global epidemiological data for MERS is shown in table 1.8
In a study conducted in the United Arab Emirates, 651 fecal and serum samples of Camelus dromedarius species of camels were tested using RT-PCR. MERS-CoV was discovered in 59.8% of the serum samples and 1.53% of the fecal samples. Analyses using anti-MERS-CoV antibodies showed that 98–100% of camels were positive for MERS-CoV. The prevalence of MERS-CoV in camel shepherds and slaughterhouse workers was 15 and 23 times higher than in the general population, respectively. Therefore, it can be inferred that camels are the primary hosts for MERS-CoV.9
Studies have shown that the MERS-CoV virus can enter cells via endosomal pathways.10 Protease enzymes like Furin can also facilitate the merging of the virus with the host cell.12 The dipeptidyl peptidase 4 (DPP4, also known as CD26), is the cellular receptor for MERS-CoV that enables the viral genome to enter the host cell cytoplasm. This receptor is most commonly found in the cells of the respiratory tract epithelium; kidney, small intestine; liver, and prostate; and activated leukocytes.14
The average incubation period for MERS is five to six days. However, it is longer in immunocompromised patients or those with comorbidities.
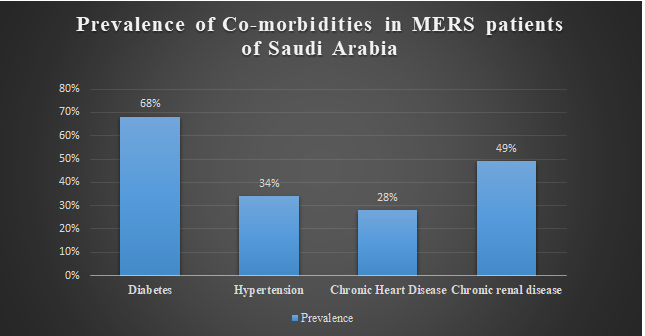
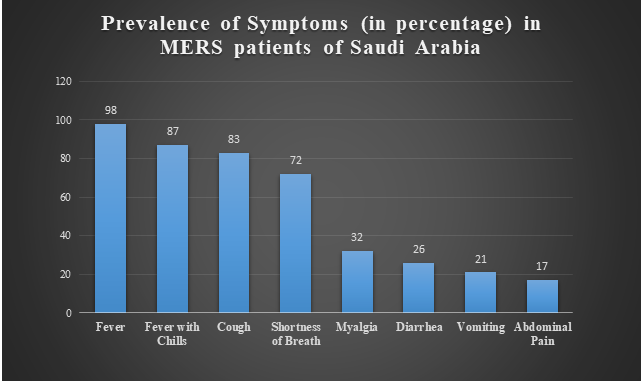
In a study reported from Saudi Arabia, a CFR of 60% was reported amongst 47 patients (46 adults and one child) with laboratory-confirmed MERS. Moreover, the case-fatality rate was higher in the elderly. Only two of the 47 patients had previously been healthy. The vast majority of patients (45 [96%]) had underlying medical conditions as shown in Figure 1. The clinical symptoms are listed in Figure 2.11
As per some studies, many hCoVs (human coronaviruses), including MERS-CoV, encode several proteins that allow them to elude the host immune system.1 The functioning of effector T-cells is inhibited, hampering the mechanism of antigen presentation. Furthermore, inflammatory cytokines (IL-1 and IL-1) and the neutrophil chemoattractant chemokine IL-8 (CXCL8) are over-expressed in MERS-CoV infected patients’ lower respiratory tracts. So, their titers rise, creating a cytokine storm that damages the infected tissues.13
It was also found in the study reported from Saudi Arabia that the chest radiography of all patients had abnormal findings, ranging from subtle to extensive unilateral and bilateral abnormalities. Laboratory tests revealed elevated levels of lactate dehydrogenase (23 [49%]) and aspartate aminotransferase (7 [15%]), along with thrombocytopenia (17 [36%]) and lymphopenia (16 [34%]). Other hCoVs, however, cause similar changes in the human body. Hence, these tests cannot be considered diagnostic of MERS.11
From the above discussion, we can conclude that MERS is associated with high mortality among hospitalized patients, particularly those with medical comorbidities. The symptoms of this disease closely resemble many other bacterial and viral respiratory infections with non-specific radiological findings.
However, we still do not have appropriate vaccines and therapeutics to prevent and treat this disease. Moreover, the disease, which was once localized in Middle Eastern countries, has now spread to over 27 other countries worldwide. Major gaps still exist in our understanding of the epidemiology, population prevalence, and clinical range of infection and disease that must be addressed immediately. Otherwise, we might be helpless in the face of another viral outbreak.
5 . World Health Organization. MERS outbreak in Republic of Korea 2015. who.int. Accessed on 21 July 2022. https://www.who.int/westernpacific/emergencies/2015-mers-outbreak
Reviewer: Priyanka
Copyright © 2025 All Rights Reserved