Post Ebola Sequelae Effects: a continuous suffering of survivors
Recent outbreaks of Ebola, Zika, dengue, Middle East respiratory syndrome (MERS), severe acute respiratory syndrome (SARS), and influenza, as well as the upcoming issue of developing antibiotic resistance, have called into question the global health system’s ability to offer adequate protection against an expanding and dynamic variety of infectious disease threats.
Certain regions in Africa often face these epidemic disease outbreaks frequently, one of which includes the Ebola virus. The Ebola virus causes the severe and usually fatal sickness known as Ebola virus disease (EVD). EVD epidemics often begin with a single case of possible zoonotic transmission, then spread from person to person by direct contact, contact with contaminated food, or contact with body fluids.1
The Ebola virus has caused multiple deadly outbreaks in Africa since it was discovered in 1976. The largest outbreak on record ever of the Ebola virus happened in West Africa in 2013-2016. This outbreak ravaged Guinea, Liberia, and Sierra Leone, with a total of 30,000 infected people recorded, including 11,000 fatalities.2
This lethal epidemic outbreak has severely impacted not only the country’s socioeconomic status but also the people or survivors of the EVD. People who survived the outbreak suffer even after the cure and face several adverse effects after their survival against the virus.
In this blog, we will briefly examine these acute and long-term adverse effects of EVD to gain a better understanding of how it impacts survivors and try to find possible treatments for the same.
To begin with, what are these adverse effects or complications?
Survivors of outbreaks are susceptible to certain clinical complications. A study done on acute EVD survivors represents the vast array of these clinical complications, including fatigue, numbness in feet, numbness in hands, headache, hearing loss, joint pain, muscle pain, and vision problems. This study concluded the fact that these post-EVD complications appear in the majority of the survivors’ population and remain present for up to 4 years.3
To briefly understand the complications, prevalence, incidences, and duration, we’ll discuss two research studies done, one on adults and one on pediatric patient survivors.
The effects of Post-EVD on adult survivors: Are they still suffering?
Researchers did a longitudinal analysis on 802 EVD survivors to understand the long-term EVD sequelae among the people of Guinea. This study was based on the clinical symptoms recorded for 48 months with their start and end dates. In it, each factor, including prevalence, incidence, and duration of the post-EVD complications or sequelae, was calculated.
The results showed that even if the prevalence and incidence of such symptoms reduced over time, the sequelae remained present for 48 months after survivors’ discharge from the Ebola treatment center. The graph below represents the result data.
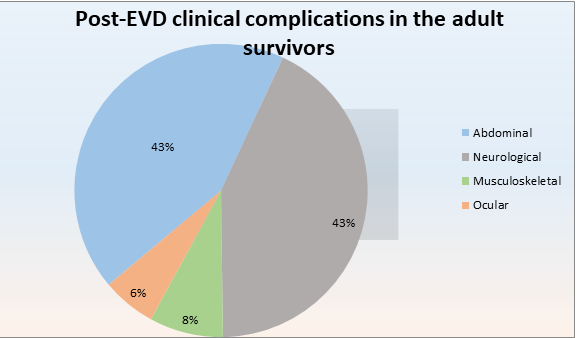
These numbers showed that 30.68% of survivors faced abdominal symptoms, 30.55% of survivors accounted for neurological complications, 5.80% for musculoskeletal, and 4.24% for ocular dysfunctions.
Out of all these patients, half of them (50.70%) reported having general symptoms two years after discharge, whereas 25.35% of this population complained four years post-discharge.
These findings conclude the fact that regular and long-term follow-up for EVD survivors is necessary even after they have been cured of the EVD infection.4
But is anyone aware of the child survivors? What adverse effects are they facing?
The aspect of the long-term health effects of EVD child survivors is almost negligible. There’s limited research data regarding this subject. However, a study conducted in Sierra Leone among child survivors has proven to shed some light on the matter.
In this study, a total of 159 EVD child survivors were recruited, with a number of 303 close contacts of those children in western and eastern Sierra Leone. Their self-reported and demographic symptoms were analyzed using stepwise logistic regression.
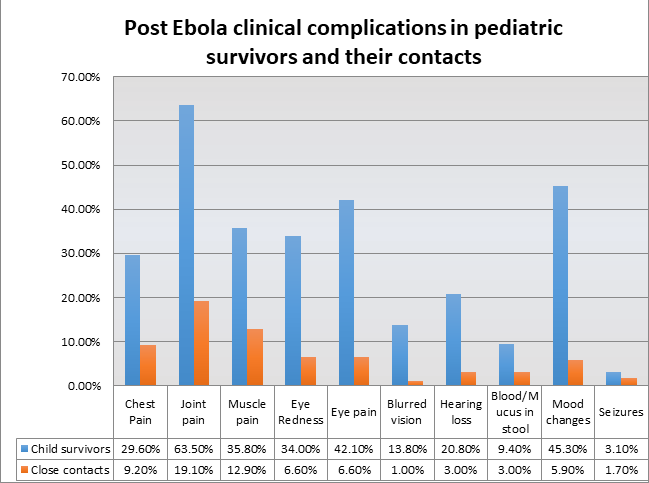
According to the results, out of total EVD child survivors, 29.6% of them showed chest pain clinical symptoms, 63.5% showed joint pain, 35.8% accounted for muscle pain, 42.1% for eye pain, 13.8% for blurred vision, 33% for hearing loss, 5% for hearing loss, and 15% accounted for blood or mucus in stool. However, in their close contact, these figures were lower.
This study concluded the fact that after a year or more than a year of post EVD, child survivors have higher chances of getting clinical complications like musculoskeletal, auditory, ophthalmic, and neurological impairment. It is suggested that to avoid the long-term disability of child survivors, routine checkups and screenings, treatments, and monitoring of these symptoms are required.5
What are the treatment options for these symptoms?
Currently, there are minimal treatments available for EVD. However, two treatments are available to cure this illness, including Inmazeb and Ebanga monoclonal antibody drugs.6
In the case of post-EVD clinical symptoms, the World Health Organization has generated an Interim Guidance for Survivors of EVD. This guidance includes various treatment and preventive methods or procedures for EVD survivors. Some of these include follow-up of the EVD survivors (first after ETU [Ebola treatment unit] discharge and subsequent follow-up visits), recommended evaluation and clinical management (for musculoskeletal, ocular, auditory, abdominal, neurological, mental health, and sexual health), consideration for special populations (pregnant women, pediatric patients), persistent Ebola virus infection in survivors, and much more.7
Conclusion
The above discussion shows the adverse effects that EVD survivors still have to face even after suffering through the infection. These clinical complications or sequelae have severely impacted the survivors’ lives to the point that a proper treatment methodology is necessary. This indicates the need for good healthcare practices to be pursued and a specific method or a way to provide patient care.
References
- Jacob ST, Crozier I, Fischer WA 2nd, et al. Ebola virus disease. Nat Rev Dis Primers. 2020;6(1):13. Published 2020 Feb 20. doi:10.1038/s41572-020-0147-3
- Furuyama W, Marzi A. Ebola Virus: Pathogenesis and Countermeasure Development. Annu Rev Virol. 2019;6(1):435-458. doi:10.1146/annurev-virology-092818-015708
- Tozay S, Fischer WA, Wohl DA, et al. Long-term Complications of Ebola Virus Disease: Prevalence and Predictors of Major Symptoms and the Role of Inflammation. Clin Infect Dis. 2020;71(7):1749-1755. doi:10.1093/cid/ciz1062
- Diallo MSK, Toure A, Sow MS, et al. Understanding Long-term Evolution and Predictors of Sequelae of Ebola Virus Disease Survivors in Guinea: A 48-Month Prospective, Longitudinal Cohort Study (PostEboGui). Clin Infect Dis. 2021;73(12):2166-2174. doi:10.1093/cid/ciab168
- Amuzu C, James PB, Bah AJ, Bayoh AVS, Singer SR. Post-Ebola sequelae among Ebola child survivors in Sierra Leone. BMC Pediatr. 2021;21(1):482. Published 2021 Oct 30. doi:10.1186/s12887-021-02957-w
- Centers for Disease Control and Prevention. Treatment. Cdc.gov. Updated 26 February, 2019. Accessed 21 July, 2022. https://www.cdc.gov/vhf/ebola/treatment/index.html#:~:text=There%20are%20currently%20two%20treatments,combination%20of%20three%20monoclonal%20antibodies
- World Health Organization. Clinical care for survivors of Ebola virus disease. Apps.who.int. Published on 11 April, 2016. Accessed on 21 July, 2022. https://apps.who.int/iris/bitstream/handle/10665/204235/WHO_EVD_OHE_PED_16.1_eng.pdf
Author: Priyanka
Reviewer: Manisha