In April 2022, an outbreak of Rift Valley fever (RVF) was reported in 8 of the 18 provinces of the Republic of Burundi, with nearly 500 reported cases in livestock, leading to a significant economic impact on livestock farmers.1 But what exactly is Rift Valley fever?
RVF is a mosquito-borne viral zoonotic disease that causes an acute viral hemorrhagic fever in livestock, leading to significant losses. The disease is caused by the Rift Valley fever virus (RVFV), a member of the genus Phlebovirus in the order Bunyavirales.2
Though the disease primarily affects animals, humans can become infected through contact with infected animals’ blood, body fluids, or tissues or by being bitten by infected mosquitoes. The spread of viruses from person to person, on the other hand, has not been documented.2 However, according to recent studies, the RVF virus has the potential to trigger global outbreaks.3
Most people infected with RVF are asymptomatic or show a mild illness with fever, weakness, back pain, and dizziness. However, about 8–10% of patients develop severe symptoms like eye disease, hemorrhagic fever, and encephalitis.2
Even though the case fatality rate (CFR) associated with RVF is less than 1%, about 50% of patients who develop hemorrhagic fever die within 3 to 6 days after the onset of symptoms. Besides, death is uncommon in patients with ocular complications, yet 50% of patients who develop lesions in the macula of the eye will experience a permanent loss of vision. Also, severe and long-term neurological deficits can occur in 1% of cases (even after more than 60 days).5 In addition, RVF has been associated with widespread abortions in infected livestock. What about humans? Is RVFV a serious threat to infected pregnant women and their unborn children? 4
In this article, we will examine the risk that RVF poses to pregnant women and their fetuses.
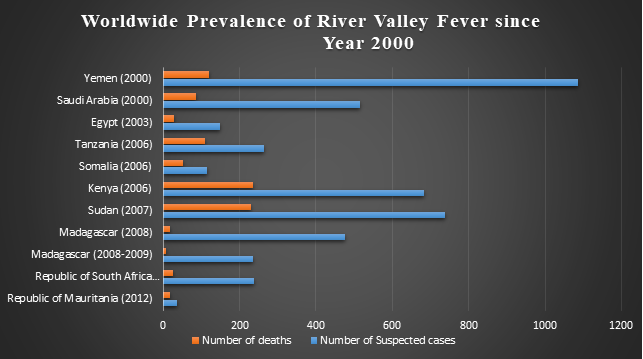
The first RVF outbreak was reported in Kenya in 1930. The virus was endemic only in Africa until 2000, when the first major RVF outbreak outside of Africa occurred in the Arabian Peninsula. The virus has now spread to other Asian and American countries as well. The prevalence of Rift Valley fever outbreaks since 2000 is shown in figure 1.5
In 2016, a suspected case of yellow fever, which was ultimately diagnosed as RVF, was brought into China. Moreover, accidental laboratory infections with RVF have been reported in non-endemic countries such as the United States of America (USA) and the United Kingdom (UK).7
In a study conducted at a governmental hospital in Port Sudan, Sudan, between June 30, 2011, and November 17, 2012, it was discovered that 15 (54%) of 28 women with an acute RVFV infection miscarried, compared to 12 (12%) of 102 women who tested negative for RVFV (p<0.0001).
In a multiple logistic regression analysis for this study, after adjusting for age, hemorrhagic disease, and chikungunya infection, the odds ratio was 7.4 (95% confidence interval [CI] 2.7–20.1; p<00001), indicating that the RVFV is a significant risk factor for causing miscarriage in infected pregnant women. In fact, this was the first study to reveal a significant correlation between RVFV and miscarriage in pregnant women.4
In another study, 30 Texel-Swifter mix-bred ewes that had previously delivered healthy lambs were injected with a highly virulent strain of RVFV at 55 or 78 days of pregnancy. Following infection or abortion, the ewes were executed. Their tissues were collected during autopsy and analyzed by polymerase chain reaction (PCR), viral isolation, and immunohistochemistry.
The results showed that RVFV replicates in maternal placental epithelial cells before infecting the fetal trophoblasts. Moreover, the virus bypassed the maternal epithelial cell barrier by directly targeting fetal trophoblasts in the haemophagous zone of the ovine placenta (an area of the placenta where maternal blood comes into direct contact with fetal cells). It induced extensive necrosis of placental tissues, resulting in hemorrhage and miscarriage.
Experiments on human placental explants revealed that RVFV multiplies efficiently in both cytotrophoblasts and syncytiotrophoblasts. It bypassed the ovine placental barrier, ultimately resulting in placental and fetal demise followed by abortion. This study highlights the risks of RVFV infection during human pregnancy.6
This research data highlight the risk posed by RVFV to pregnant women and their fetuses. Hence, the spread of this virus must be stopped or contained to ensure the safety and quality of life of pregnant women and their children living in endemic Africa or other infected areas.
Mosquitoes serve as both a reservoir and a vector for RVFV, transmitting the virus to both animals and people. As the number of RVFV-infected mosquitos increases during the rainy season and floods, so does the number of RVF cases.2
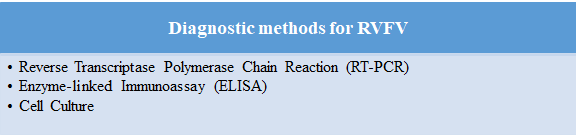
The incubation period for RVF may range from 2 to 6 days.5 Since its symptoms are non-specific, the disease can only be confirmed by the following methods:
However, even after a thorough diagnosis, the lack of FDA-approved RVF therapies limits the provided care to supportive treatment, particularly in critical cases. Hence, RVF can cause significant morbidity and mortality in patients with severe symptoms.2
It is evident from the above discussion that RVF can cause fetal death in infected women. Hence, appropriate preventive measures should be implemented to prevent the spread of infection to humans, especially pregnant women. Mass vaccination of animals in endemic areas and prevention of breeding mosquitoes could help reduce the spread of infection to humans. Moreover, laboratories in endemic areas should be upgraded with adequate diagnostic facilities to ensure timely virus detection. In addition, efforts should be made to develop appropriate preventive and therapeutic interventions to combat RVF. The world is counting on medical research to avoid another epidemic spreading in the future.
Reviewer: Priyanka
Copyright © 2025 All Rights Reserved