We have seen the emergent spread of Zika virus into huge subgroups of immunologically naive human populations in past few years. The World Health Organization (WHO) declared the Zika virus (ZIKV) outbreak in South America, as well as the related increase in neurological diseases and infant abnormalities, a “public health emergency of worldwide concern” in February 2016. Later on, the Centers for Disease Control and Prevention (CDC) in the United States and the World Health Organization (WHO) agreed that there was adequate evidence to suggest a causal association between maternal ZIKV infection and congenital Zika syndrome (CZS) in offspring.1
The Zika virus is a flavivirus that is spread to humans mostly by the bite of an infected mosquito of the genus Aedes. It was discovered in monkeys in 1947. Outbreaks of the Zika virus have been documented in Africa, the Americas, Asia, and the Pacific. From the 1960s until the 1980s, rare sporadic cases of human infections were discovered in Africa and Asia, usually accompanied by moderate symptoms.
Sexual transmission and Zika virus transfer from mother to the fetus have also been recorded. Congenital Zika virus infection can result in serious brain and eye defects and has been linked to neurodevelopmental issues in newborns, such as seizures, joint contractures, swallowing difficulty, visual impairments, and hearing loss.2
In this blog, we will explore the link between ZIKV and how it can affect pregnant women. Let’s begin by understanding what the possible adverse outcomes are.
Researchers analyzed infants delivered to people infected with Zika during pregnancy in US territory in the August 2018 Vital Signs Report. One in every seven newborns (14 percent) had one or more documented health concerns probably caused by Zika.3
Babies with possible Zika infection can develop long term health problems as they grow.
During the Zika virus outbreak in Colombia from June 2015 to July 2016, the presence of ZVD was reported to the national monitoring system in over 18,000 pregnant women. Two percent of the children or fetuses born to women with laboratory-confirmed ZVD had a brain or eye abnormality.
In another report, it was found that the majority (84%) were born with brain abnormalities and/or microcephaly (small head size); while almost two-tenths (16%) had eye abnormalities but no brain abnormalities.2
Other than these ZIKV is also linked with complications like pregnancy loss, low birth weight and pre term birth.
Let’s have a look at the data collected by various reports to understand the Zika-associated birth abnormalities
In national surveillance, data were collected regarding the incidence of ZVD (Zika Virus Disease) that were reported over a period of time. A subset of these women tested positive for Zika virus RNA using a real-time reverse-transcriptase-polymerase-chain-reaction (rRT-PCR) assay.2
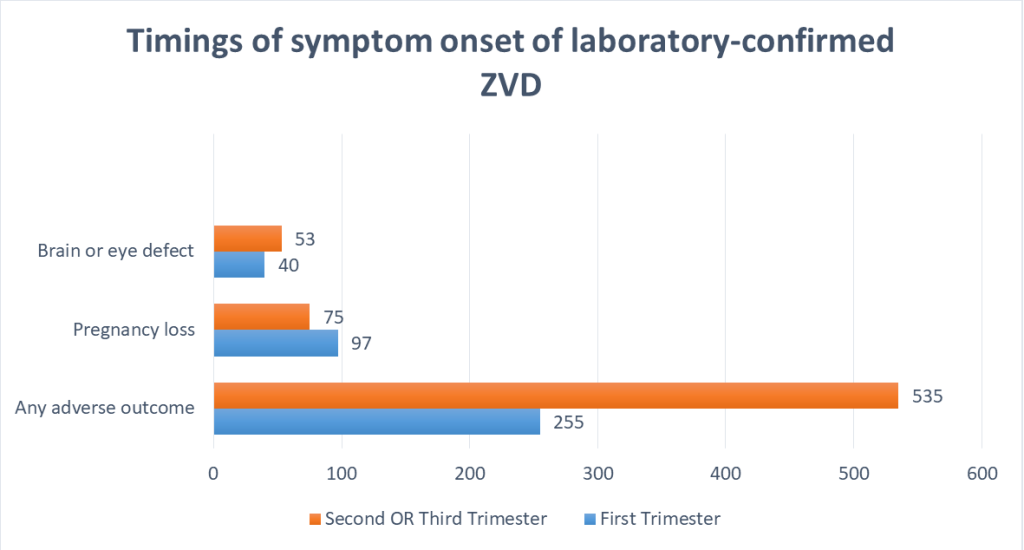
According to a study, 790 (14%) of the 5673 pregnancies experienced at least one negative outcome. Brain or eye abnormalities were documented in 93 newborns or fetuses (2%), with 75 (81%) in live births and 18 (19%) in pregnancy losses. The percentage of brain and eye problems was greater in women whose symptoms began in the second or third trimesters than
in those who began in the first trimester.2 The graph below represents the timings of these symptoms onset of laboratory-confirmed ZVD.
Approximately 1 in 20 (5.3%) persons with Zika virus infection during pregnancy had a baby with Zika-associated birth abnormalities, compared to around 1 in 25 (4.2%) people without Zika virus infection during pregnancy.4
Case reports from countries with endemic transmission, such as Vietnam, have arisen as a result of increased awareness of the teratogenicity of ZIKV infection during pregnancy.
Furthermore, two older children in the United States have a phenotype consistent with congenital Zika syndrome; their mothers lived in a country with endemic ZIKV transmission, had symptoms of ZIKV infection in the first trimester of the pregnancy, as well as laboratory evidence of previous ZIKV infection in maternal specimens collected years after the pregnancy.
Data reveal that in regions where ZIKV infection is a threat, the virus has been having a teratogenic effect on fetuses for many years, but the impact has not been identified. These findings establish a relationship between ZIKV and birth defects.
There is no vaccination available to help protect against the Zika virus. As WHO has declared a public health emergency of international concern for the second time in two years, the vaccination efforts have been accelerated. There are many potential candidates in the pipeline such as NIAID’s Vaccination Research Center scientists created a DNA-based vaccine (VRC). This VRC 705 trial has assessed the appropriate dosage for delivery as well as the vaccine’s safety and immunogenicity. Another candidate is ZPIV, a purified inactivated Zika vaccine produced by the Walter Reed Army Institute of Research (WRAIR) 5. These can be promising vaccine the trial has been completed but further testing is required. Besides all these efforts on developing a Zika vaccine, it may not be accessible to the public for another year or two.
If someone is pregnant or trying to conceive, avoid travelling to a Zika-affected location unless absolutely necessary. If anyone has to travel, they should consult with their physician about how to protect themselves from Zika. This also involves utilizing a barrier method of birth control and avoiding mosquito bites.
Since there isn’t any particular therapy for ZIKV, one can manage the symptoms by taking acetaminophen (Tylenol®) to relieve fever and discomfort if they get sick. To limit the risk of bleeding, avoid using aspirin and other non-steroidal anti-inflammatory medications (NSAIDS) until dengue has been ruled out. Moreover, if a person already taking medication for another medical condition, see a doctor before introducing another medication.6
As the above discussion has demonstrated, there is sufficient evidence to establish a relationship between ZIKV and birth defects. Although more data and research are needed before making any conclusions, we can fight this battle with the combined efforts of researchers and being aware ourselves. Until a vaccine is developed, we must take preventive measures to protect ourselves, especially pregnant women and women trying to conceive.
Reviewer: priyanka
Copyright © 2025 All Rights Reserved