
Asian countries have been facing cancer burden with the highest incidences as well as the highest mortality rate. In this white paper, we have presented region-wise cancer incidences and death rates. The use of cancer treatments in real life is very different from the use of treatments in clinical studies, as in clinical studies, patients are kept under strict monitoring to check compliance with treatment and other procedures. To keep an eye on the real world for treatment compliance, the quality of cancer care must be evaluated. Throughout the entire cancer treatment process, there are a number of potential failure points as well as some difficulties that patients must overcome. In the entire scenario, it becomes very important to evaluate the quality of cancer care being received by individuals. Certain endorsed strategies ensure the quality of cancer care, and these measures are described simply and concisely in this white paper.
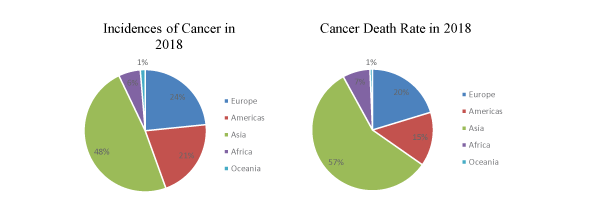
Despite substantial progress in cancer research, it is still one of the leading causes of death andhas been proving a burden in society. Asian countries have been facing cancer burden with the highest incidences as well as the highest mortality rate. Following figures are showing the country-wise incidences and mortality rate.
A newly released RAND Health study has reported that in the United States (US), 1 among the 7 patients with breast cancer has the chances of missing cancer care they are receiving. The corresponding number for colorectal cancer is 1 among the 5 patients. A report was issued in 1999 by the Institute of Medicine (IOM) that reported state-of-the-art care was not being received by the cancer patients. Many oncologists were surprised with the results of this report as there was much improvement in the cancer treatments at that time too.
It was realized that the use of treatments in the real life is very different from the use of treatment in the clinical studies as in clinical studies patients are kept under strict monitoring to check the treatment and other procedures compliance. This is still happening in the current scenario.
To keep an eye on the realworld for treatment compliance, the evaluation of the quality of cancer care is necessary. The Institute of Medicine (IOM) has defined the quality of care as “the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge” (IOM, 1990).
In simple terms, poor quality may be due to too much unnecessary care (eg, unnecessary medications, tests, or procedures associated with risks and adverse events), too little care, or inappropriate care (eg, use of contradictory medicines together, poor surgical methods). Good quality means providing patients with appropriate services in a technically competent manner, with good communication, shared decision making, and cultural
sensitivity. In most developed countries, measuring the quality of cancer care is an integral part of cancer care, with detailed investigations revealing that not all patients are receiving optimal care and maximum survival benefit from the most up-to-date cancer treatments. The quality of cancer care mainly ensures that the care is effective, safe, patient-centered, efficient, timely, and equitable.




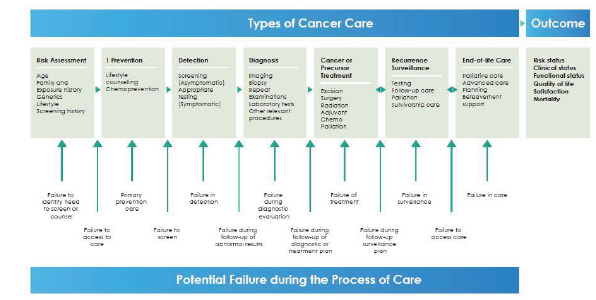
Different steps at which cancer care is required include risk assessment, primary prevention, screening, detection, diagnosis, treatment, recurrence surveillance, and end-of-life care. Risk assessment is based on environmental exposures such as lead, familial factors such as genetic risk, and lifestyle factors such as smoking.
Primary prevention denotes counseling related to lifestyle behaviours, including diet, smoking, exercise, alcohol use, and chemoprevention. Health care professionals may implement efficient and effective strategies to evaluate high-risk behaviours and help people to modify them. Prevention strategies include education and counseling, referrals to related professionals and support groups or community agencies such as nutritionists, and pharmacotherapy prescriptions for quitting smoking. Testing for precursors or cancer may be asymptomatic (screening) and/or symptomatic. If the results are abnormal, a diagnostic evaluation is required, and if a precancerous or cancerous condition is discovered, the treatment step is taken. After completion of treatment, lifelong surveillance must be performed to identify recurrence, new cancers, and manage long-term adverse events. Because 50% of cancer patients ultimately die, quality-of-life care is also necessary.
The cancer care failures fall into two types: (a) failure in specific care delivered to patients at different points in their cancer history; and (b) failure between these types of care during the transitions, as shown in the below figure. The types of cancer care provided and the transitions between them are collectively called “Processes of care”. Previously, clinicians and healthcare professionals focused primarily on the types of cancer care available, but flaws in the transitions between them are equally important. Because the main objective of cancer care is to improve short- and long-term patient and system outcomes, improvement in the entire process of care is required.
There are a number of barriers to cancer care. The main barriers among them are described in this section.
Innovative ideas are needed to improve cancer care coordination for patients suffering from the disease to improve patient experience of care, achieve better care outcomes, and lower cost.
Establishing a quality surveillance system can aid in detecting disparities and gaps in care delivery. This will help the health-care providers improve their services as well as allow policy-makers to target areas requiring improvement in cancer control plans. The quality of cancer care will automatically improve if healthcare professionals focus on the triple aim of health care, ie, improving the health of populations, improving the experience of care, and reducing the per capita costs of health care. Many professional organizations currently have programs to measure cancer care quality. The following measures are used extensively to measure the quality of cancer care:
Outcome measures, often considered as key indicators of health care quality, assess the results of health care with respect to recovery, survival, and functional restoration. For patients with cancer, survival is the most important outcome and therefore the primary concern. In addition to this, cancer patients must understand the immediate and long-term effects of the disease and its treatment.Earlier, outcome measures were focused on the short-term results of cancer care, primarily on mortality and post treatment complications.That focus has now been expanded to include immediate and intermediate findings related to the quality of life during and post treatment, including symptom management and functional status. The measures supported by the National Quality Forum include some cancer-specific outcome measures, reflecting the challenge of measuring the long-term outcomes for cancer patients. Suggested areas for outcome measure development for cancer patients include measures reflecting patients’ preferences and compliance with treatment therapies, eg, the measure of the patients’ assessment of their quality of life during and after treatment.
These measures evaluate the adequacy of health care provision settings, together with the physical facilities in which the care is provided and the individuals who engage in providing that care, eg, nurse-to-patient ratios, key technologies such as robotic surgery, and patient services such as palliative care. Few of the structure measures supported are specific to cancer, which reflects the general shortfall of structure guidelines for cancer care.
Process measures evaluate the adherence to standards of care where evidence connects a specific approach with improved outcomes. More than ninety process measures relevant to cancer patients have been supported up to this point, such as screening elderly patients for fall risk or administering antibiotics before surgery to prevent surgical site infections; however, few are cancer-specific.
Efficiency measures assess the connection between inputs and outputs in health care delivery, comparing the use of resources and related costs with the level of achieved health outcome, eg, the time between the diagnosis of the disease and the start of treatment. There are many ongoing projects to expand supported efficiency measures.
Cost-of-care measures assess the total direct and indirect costs related to a specific health care service or care episode. These measures provide insights into perceived cost inefficiencies and increased costs related to comorbidities, treatment settings, delayed diagnoses, and adverse events. When there are greater costs noted for some treatment settings, such as comprehensive cancer centers and research-oriented medical centers, further investigations of the clinical outcomes are needed. Despite the critical observations on rising health care costs, gaps are still present in the supported measures, in both the health cost-of-care measures and care cost information
Patients’ perception-of-care measures assess patients’ satisfaction with the health care they received. Although restoration of health is a priority among patients and providers, equally important is patient satisfaction throughout the period of care. This is particularly true for cancer patients, whose treatment may be non-curative. Most providers use the endorsed Hospital Consumer Assessment of Systems survey and healthcare providers to assess patient satisfaction. This survey is applicable to inpatient care only, is not specific to cancer, and does not evaluate the quality of life during and post treatment. This represents a big gap because cancer treatment is provided mostly in an outpatient setting, and many patients receive all treatment cycles without an inpatient hospital stay. These measures can be expanded to include tools that will assist providers in delivering patient-directed and patient-centred care, regardless of the health care
setting.
Good cancer care is dependent on the decisions and actions of both health care professionals and individual patients during the multiple processes of care. However, their actions usually depend on organized support systems. If administrative and clinical leaders wish to improve cancer care, they have to develop organizational strategies for the elements affecting clinical performance. Gaps in health professionals’ information and skill must be addressed by decision support strategies, which include the establishment of a process and structure to develop, disseminate, and update (when required) clinical practice guidelines.
Reviewer: Manisha
Copyright © 2025 All Rights Reserved